Improving the STS score model for predicting postoperative complications after coronary artery bypass grafting: A study on diagnostic accuracy
ORIGINAL RESEARCH ARTICLE
Improving the STS score model for predicting postoperative complications after coronary artery bypass grafting: A study on diagnostic accuracy
Article Summary
- CARDIOVASCULAR DISEASES
- Published: 14/07/2026
- Received: 26/04/2026
- Revised: 21/06/2026
- Accepted: 22/06/2026
- Views: 30
- Downloads: 10
- Keywords: STS score, coronary artery bypass surgery, complications, left ventricular diastolic dysfunction, left atrium, prognosis, diagnostic accuracy
Address for Correspondence: Ishen K. Moldotashev, Adam University, Bishkek, Kyrgyz Republic
Email:
ORCID: Asan K. Nasarov A. - 0000 – 0002 – 6949 – 2678; Taalaibek Z. Kudaiberdiev - 0000 – 0002 – 3669 – 066X; Ishen K. Moldotashev - 0000 – 0001 – 5525 – 3599; A.A. Sorokin - 0000 -0002 – 9682 – 8085
Asan K. Nazarov1, Taalaibek Z. Kudaiberdiev2, Ishen K. Moldotashev3, A.A.Sorokin4
1Bicard Cardiosurgical Clinic, Bishkek, Kyrgyz Republic
2Center of Research and Postgraduate Education, Bishkek, Kyrgyz Republic
3Adam University, Bishkek, Kyrgyz Republic
4I.K. Akhunbaev Kyrgyz State Medical Academy, Bishkek, Kyrgyz Republic
Abstract
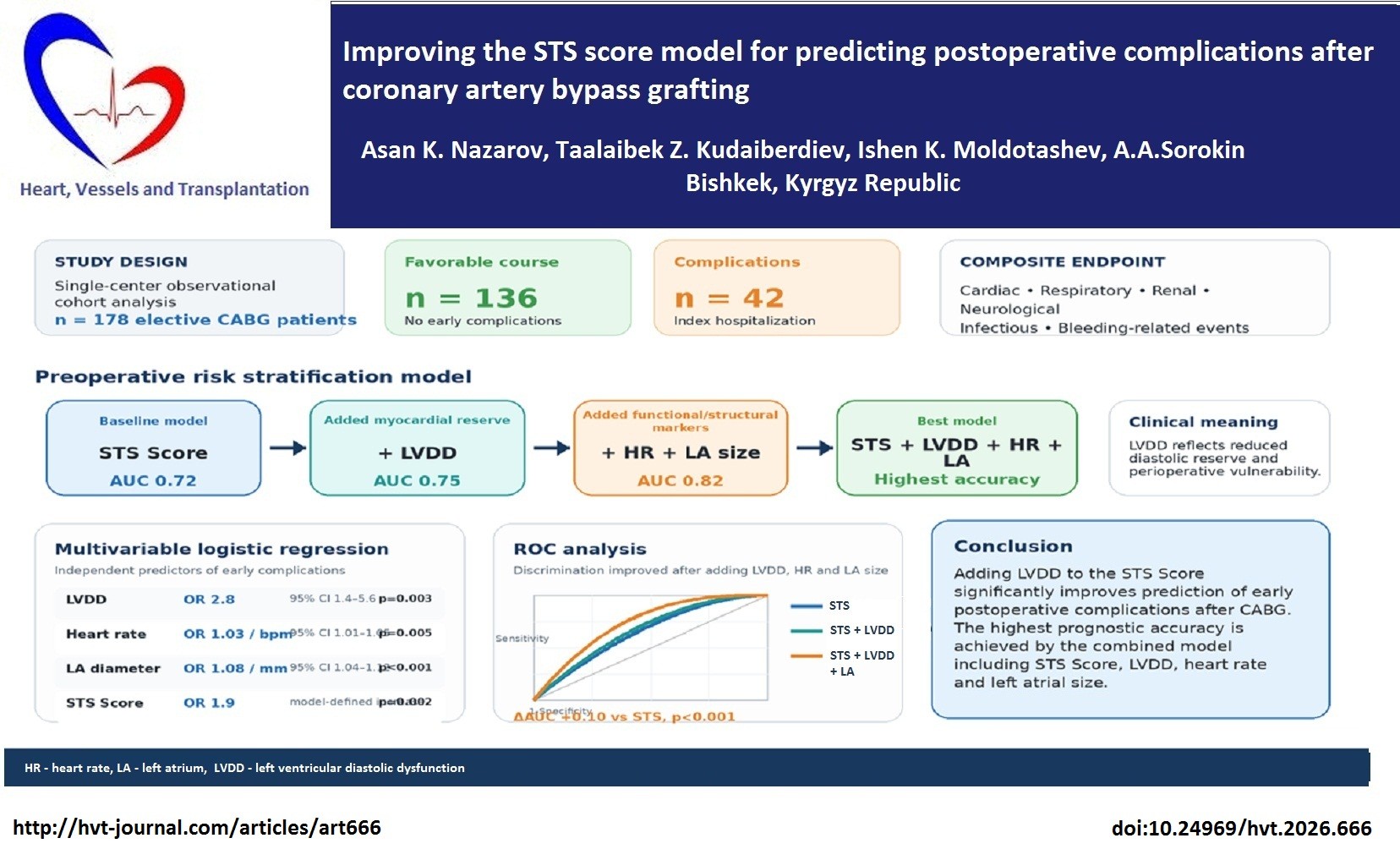
Objective: To improve the accuracy of predicting early postoperative complications in patients with coronary artery disease (CAD) who underwent elective coronary artery bypass grafting (CABG) by supplementing the STS Score with indicators of left ventricular diastolic dysfunction (LVDD), heart rate (HR), and left atrial (LA) size.
Methods: This single-center observational cohort analysis included 178 consecutive adult patients with CAD who underwent elective CABG. Preoperative clinical, laboratory, electrocardiographic, echocardiographic, and functional parameters were analyzed. Depending on the early postoperative course during the index hospitalization, patients were stratified into a favorable-course group (n=136) and a postoperative-complications group (n=42). The primary outcome was a composite of early postoperative complications, including cardiac, respiratory, renal, neurological, infectious, and bleeding-related events requiring additional treatment or prolonging intensive care or hospital stay. LVDD was diagnosed by a multiparametric Doppler echocardiographic approach according to contemporary recommendations, including mitral inflow parameters, tissue Doppler e′ velocity, average E/e′ ratio, tricuspid regurgitation velocity, and LA size/volume where available. Logistic regression and ROC analysis were used to identify predictors of complications; ROC curves were compared using the DeLong method.
Results: LVDD was identified as an independent and clinically significant predictor of early postoperative complications after CABG. The STS score demonstrated moderate discriminative ability (AUC 0.72; 95% CI 0.64–0.80). The addition of LVDD to the STS score model significantly improved predictive performance (AUC 0.75; 95% CI 0.68–0.83; ΔAUC=+0.03; p=0.041). The inclusion of HR and LA size resulted in further significant improvement (AUC 0.82; 95% CI 0.75–0.88; ΔAUC=+0.10; p<0.001).
Conclusion: LVDD reflects reduced diastolic reserve and increased vulnerability to perioperative hemodynamic stress, which are not fully captured by traditional risk scores. Adding LVDD to the STS score provides a statistically significant improvement in predicting early postoperative complications after CABG. The highest prognostic accuracy is achieved using a combined model that includes STS score, LVDD, HR, and LA size.
Key words: STS score, coronary artery bypass surgery, complications, left ventricular diastolic dysfunction, left atrium, prognosis, diagnostic accuracy
![]()
![]()
Graphical abstract
Introduction
Coronary artery disease (CAD) occupies a leading position in the structure of morbidity and mortality and remains one of the key medical and social problems of modern healthcare, accounting for a significant proportion of disability and economic costs (1, 2). Despite advances in pharmacological therapy and interventional technologies, CABG continues to be considered one of the most effective methods of surgical myocardial revascularization in patients with multivessel CAD, left main CAD, diabetes mellitus, and reduced left ventricular ejection fraction (LVEF) (3).
At the same time, postoperative complications after CABG remain a serious clinical problem affecting early and long-term survival, length of hospital stay, and treatment costs (4). The spectrum of complications includes cardiac, respiratory, renal, infectious, bleeding-related, and cerebrovascular events that significantly worsen prognosis (5–9). Early prediction of such complications is therefore important for risk stratification, perioperative planning, and targeted preventive measures.
In clinical practice, prognostic risk scores such as EuroSCORE II, MAGGIC, and the STS score are used to assess surgical risk (10–12). However, traditional models may have limited discriminatory ability when applied to different populations and to composite postoperative morbidity endpoints (13, 14). One limitation is that most models predominantly include demographic, comorbid, and operative variables, while myocardial functional reserve – particularly left ventricular diastolic dysfunction (LVDD) - may be insufficiently represented (15).
LVDD is a multiparametric echocardiographic condition reflecting impaired myocardial relaxation, reduced ventricular compliance, increased filling pressure, or a combination of these mechanisms. Importantly, abnormal relaxation and elevated filling pressure may have different clinical and prognostic implications. In the setting of CABG, patients with impaired diastolic reserve may be more vulnerable to perioperative fluctuations in preload and afterload, myocardial ischemia-reperfusion injury, systemic inflammation, and volume overload. Therefore, LVDD may add prognostic information to traditional surgical risk scores, especially in patients with preserved or moderately reduced LVEF (16, 17).
Among the available risk models, we selected the STS score as the baseline model because it is focused on perioperative risk assessment and is widely used in cardiac surgery. Unlike EuroSCORE II, which primarily predicts mortality, and MAGGIC, which focuses on long-term outcomes in heart failure, the STS score better reflects early postoperative risk.
However, LVDD, heart rate (HR), and left atrial (LA) size are not directly incorporated into the standard STS
questionnaire.
The aim of this study was to improve the accuracy of predicting early postoperative complications in patients with CAD who underwent elective CABG by adding LVDD, HR, and LA size to the STS score model.
Methods
Study design and population
This was a single-center prospective observational cohort study on diagnostic accuracy and prognostic significance of a modified STS-based model with inclusion of LVDD, HR, and LA size in prediction of early postoperative complications after elective CABG. The manuscript was checked for compliance with STROBE reporting principles for observational studies and with STARD principles applicable to diagnostic/prognostic accuracy studies.
The study included 178 consecutive adult patients with CAD who were referred for elective CABG and underwent surgery at Bicard Cardiosurgical Clinic, Bishkek, Kyrgyz Republic. The studies were conducted from September 2021 to October 2024. B
Depending on the early postoperative course, patients were divided into two groups: patients with a favorable postoperative course (n=136) and patients with postoperative complications (n=42). The classification of postoperative complications was established before statistical analysis and applied uniformly to all patients.
Inclusion criteria were presence of clinical and angiographic indications for elective CABG; age ≥18 years; availability of preoperative clinical, laboratory, electrocardiographic (ECG), echocardiographic, and STS core data; and availability of postoperative follow-up data during the index hospitalization.
Exclusion criteria were: emergency cardiac surgery; repeat cardiac surgery; combined valve or aortic surgery; acute inflammatory or infectious disease in the preoperative period; atrial fibrillation or rhythm disturbances that made transmitral A-wave assessment unreliable; and incomplete clinical or instrumental data.
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki, including the 2024 revision, and with local institutional requirements for clinical research involving human participants. The study protocol was approved by Ethics Committee of Adam University N5, September 10, 2021. Informed consent was obtained from patients for diagnostic procedures, treatment, and surgery.
Baseline variables
Baseline variables included all parameters presented in Table 1: age, sex, body mass index (BMI), LVEF, HR, LA diameter, serum creatinine, STS Score, presence of LVDD, diabetes mellitus, prior myocardial infarction (MI), chronic obstructive pulmonary disease (COPD), smoking status, and left ventricular hypertrophy (LVH).
Before the operation, all patients underwent an ECG using the MAS-400 device, echocardiography using the ViViD 7 device, and coronary angiography using a Siemens angiographic unit according to standard methods. Postoperative events were assessed during the hospitalization using operative reports, intensive care unit records, daily postoperative notes, laboratory results, and discharge summaries.
Surgery and postoperative assessment
All patients underwent elective CABG according to standard surgical practice at Bicard Cardiosurgical Clinic. CABG was performed with cardiopulmonary bypass and cardioplegia. We recorded extent of CAD, duration of cardiopulmonary bypass time (CPB), aortic-cross-clamp time (ACCT), number of shunts, duration of hospital stay and mortality.
Echocardiography and operational definition of LVDD
Doppler echocardiography using VIVID 7 machine (?) was performed before surgery to assess left ventricular systolic and diastolic function. LVEF was measured using standard echocardiographic methods. LA size was assessed by anteroposterior LA diameter; when available, LA volume index (LAVI) was also considered.
LVDD was diagnosed using a multiparametric echocardiographic approach according to ASE/EACVI recommendations (18). The assessment included transmitral inflow parameters (E-wave velocity, A-wave velocity, E/A ratio, and deceleration time), tissue Doppler mitral annular velocities (septal e′ and lateral e′), average E/e′ ratio, peak tricuspid regurgitation (TR) velocity, and LA size or LAVI when available.
In patients with preserved LVEF, LVDD was considered present when more than half of the following parameters were abnormal: septal e′ <7 cm/s or lateral e′ <10 cm/s; average E/e′ ratio >14; LAVI >34 mL/m² or increased LA size when indexed volume was unavailable; and peak TR velocity >2.8 m/s. Diastolic function was considered normal when more than half of the parameters were normal. Cases with an equal number of normal and abnormal variables were considered indeterminate and were not classified as definite LVDD unless supported by the full clinical and echocardiographic pattern.
In patients with reduced or moderately reduced LVEF, or in patients with myocardial disease, the grading algorithm was based on mitral E/A ratio, E-wave velocity, E/e′ ratio, TR velocity, and LA size/LAVI. Impaired relaxation with normal filling pressure corresponded to grade I; pseudonormal filling with elevated filling pressure corresponded to grade II; and restrictive filling corresponded to grade III. Because the number of patients in each grade was limited and complete grade-specific data were not uniformly available, the primary prognostic analysis used a binary LVDD variable (LVDD present/absent). This approach was chosen to avoid overfitting and unstable estimates in the multivariable model.
The binary LVDD variable therefore reflected the presence of clinically meaningful diastolic dysfunction, while the Discussion separately addresses the potential difference between abnormal relaxation and increased filling pressure.
Risk scores
The integrated STS score was calculated preoperatively using the STS Adult Cardiac Surgery Risk Model (12). The STS score was selected as the baseline model because it is specifically focused on cardiac surgery and perioperative risk assessment. To avoid duplication of prognostic information, variables that are already components of the STS score were not simultaneously forced into the extended model.
Outcome variables
The primary outcome was the presence of at least one early postoperative complication after CABG during the index hospitalization. Complications were defined as clinically significant events requiring additional treatment, invasive or pharmacological intervention, prolonged intensive care monitoring, or prolongation of hospital stay.
The composite endpoint included the following event categories: Postoperative complications were assessed during the in-hospital postoperative period after elective CABG. The following complications were recorded: any cardiac rhythm disturbances, atrial fibrillation, pleural effusion, heart failure, acute kidney injury, respiratory failure, acute MI, bleeding requiring re-sternotomy and in-hospital mortality.
For the statistical analysis, the endpoint was coded as a binary variable: absence or presence of any early postoperative complication. If several complications occurred in the same patient, the patient was counted once in the complication group.
Statistical analysis
The ??? software was used for statistical analysis. The normality of distribution of quantitative variables was assessed using the Shapiro-Wilk test. Since most variables were not normally distributed, data are presented as median and interquartile range (Me (Q1; Q3)); Categorical variables are presented as absolute and relative values (n, %).
Between-group comparisons were performed using the Mann-Whitney test for quantitative variables and Pearson Chi-square test or Fisher exact test for categorical variables. Differences were considered statistically significant at p<0.05.
Risk factors for early postoperative complications were identified using univariate and multiple logistic regression analysis. The final extended model included STS score plus LVDD, HR, and LA size, because these variables are not directly included in the standard STS questionnaire and were clinically relevant in the perioperative setting.
The predictive ability of the models was assessed using ROC analysis with calculation of AUC and 95% confidence intervals. Models were compared using the DeLong test (19). Optimal cut-off values were determined using the Youden index. Reclassification was assessed using net reclassification improvement (NRI) and integrated discrimination improvement (IDI). Decision curve analysis was used to evaluate the potential net clinical benefit of the models across clinically relevant threshold probabilities.
Results
Clinical characteristics of patients undergoing CABG
The study included 178 consecutive patients undergoing elective CABG. The patients' age ranged from 31 to 84 years. Among them, there were 133 men (74.7%) and 45 women (25.3%). All patients had angina pectoris of functional class II–IV according to the Canadian Cardiovascular Society classification before the operation. Myocardial infarction was documented in 62 patients (34.8%), 51 of them (28.7%) before the operation, and the remaining 11 patients (6.2%) suffered MI immediately before the operation. None of the patients included in the study had previously undergone CABG surgery. Clinical signs of chronic heart failure (NYHA I-II grade) were present in 151 patients (84.8%). Concomitant hypertension was registered in 142 patients (79.8%). The average BMI was 30.2 (3.0) kg/m², indicating overweight in most patients. Hypercholesterolemia (total cholesterol >4.5 mmol/L) was detected in 145 patients (81.5%).
According to coronary angiography, all patients were found to have multivessel CAD (more than 3 vessels). During CABG surgery, the duration of CPB ranged from 56 to 270 minutes (mean 131.9 (53) minutes), and the duration of ACCT from 14 to 180 minutes (average 65.7 (41.0) minutes). The mean number of bypasses/ shunts per patient was 2.8 (0.4). The mean duration of patient stay in hospital was 7.5 (3.7) days. The overall hospital mortality rate was 2.2%.
The complication developed in 42 patients. The structure of complications was as follows: any cardiac rhythm disturbances — 18 patients (42.9%); atrial fibrillation — 7 patients (16.7%); pleural effusion — 6 patients (14.3%); heart failure — 5 patients (11.9%); acute kidney injury — 2 patients (4.8%); respiratory failure — 2 patients (4.8%); acute MI — 1 patient (2.3%); bleeding requiring resternotomy — 1 patient (2.3%). In-hospital mortality was observed in 4 of 178 patients (2.2%).
Characteristics of patients with and without complications
A favorable early postoperative course was observed in 136 patients, whereas 42 patients developed at least one early postoperative complication during the index hospitalization. There were no differences in mean age, sex, BMI, diabetes mellitus, prior MI, smoking, COPD and LVH in patients with an without complications after CABG.
The most clinically relevant between-group differences were observed for LVEF, LVDD, HR, LA diameter, creatinine, and STS score (Table 1). LVEF was markedly lower (p=0.002), while creatinine and STS score were significantly higher (p=0.021 and p<0.001, respectively), HR was faster (p=0.004) and LA diameter was markedly larger (p<0.001) in group of patients with complications as compared with those without. The LVDD affected significantly more patients with complications as compared to patients without complications (66.7% vs. 37.8%, p<0.001).
|
Table 1. Baseline characteristics of patients with and without complications after CABG |
|||
|
Variables |
Without complications (n=136) |
With complications (n=42) |
p |
|
Age, years |
58 (52; 64) |
61 (55; 67) |
0.15 |
|
Sex, male, n (%) |
103 (75.7) |
36 (85.7) |
0.18 |
|
BMI, kg/m² |
26.9 (24.4; 29.8) |
27.2 (25.0; 30.5) |
0.78 |
|
LVEF, % |
52 (46; 60) |
45 (40; 52.8) |
0.002 |
|
Heart rate, bpm |
74 (65; 83) |
82 (71; 91) |
0.004 |
|
LA diameter, mm |
39 (38; 43) |
43.5 (40; 47) |
<0.001 |
|
Creatinine, µmol/L |
90 (76; 107) |
97.5 (89.8; 114) |
0.021 |
|
STS Score |
0.009 (0.0065; 0.013) |
0.0158 (0.0105; 0.0397) |
<0.001 |
|
LVDD, n (%) |
51 (37.8) |
28 (66.7) |
0.001 |
|
Diabetes mellitus, n (%) |
58 (42.6) |
16 (38.1) |
0.52 |
|
Prior myocardial infarction, n (%) |
35 (25.7) |
11 (26.2) |
0.97 |
|
COPD, n (%) |
22 (16.2) |
5 (11.9) |
0.63 |
|
Smoking, n (%) |
25 (18.4) |
6 (14.3) |
0.64 |
|
LVH, n (%) |
80 (58.8) |
27 (64.3) |
0.46 |
|
Data are presented as median (interquartile range), number (%) Mann Whitney test, Chi-square or Fischer exact test BMI – body mass index, CABG – coronary bypass surgery, COPD - chronic obstructive pulmonary disease, LA – left atrial, LVDD – left ventricular diastolic dysfunction, LVEF – left ventricular ejection fraction, LVH – left ventricular hypertrophy |
|||
Predictors of complications after CABG
Multiple logistic regression analysis (Table 2) revealed that LVDD, increased HR, LA diameter and STS score were independent predictors of complications development after CABG. Complications were 2.8 times more likely to develop in patients with LVDD (p=0.003), risk of complications increased with raise in HR and increase in LA diameter (p=0.005 and p<0.001) and with every 1.9 points of STS score (p=0.002).
|
Table 2. Multiple logistic regression analysis of independent predictors of complications after CABG |
||
|
Parameter |
OR (95% CI) |
p |
|
LVDD |
2.8 (1.4–5.6) |
0.003 |
|
Heart rate |
1.03 per 1 bpm (1.01–1.05) |
0.005 |
|
LA diameter |
1.08 per 1 mm (1.04–1.12) |
<0.001 |
|
STS Score |
1.9 per model-defined increase |
0.002 |
|
CABG – coronary bypass surgery, CI – confidence interval, LA – left atrial, LVDD – left ventricular diastolic dysfunction, OR – odds ratio |
||
Diagnostic value of modified STS score in prediction of complications after CABG
ROC analysis revealed that combination of STS score and LVDD improved predictive accuracy of STS alone and LVDD alone (AUC -0.75), further addition of HR and LA increased AUC up to 0.82 (95%CI 0.75-0.88)
(Fig. 1 and Table 3).
The addition of LVDD, HR, and LA size to the STS Score improved risk classification: NRI=0.32 (p=0.002) and IDI=0.07 (p=0.001).
Decision curve analysis showed that the STS + LVDD + HR + LA model provided the greatest net clinical benefit within the threshold probability range of 10–40% compared with the STS Score and STS + LVDD models.
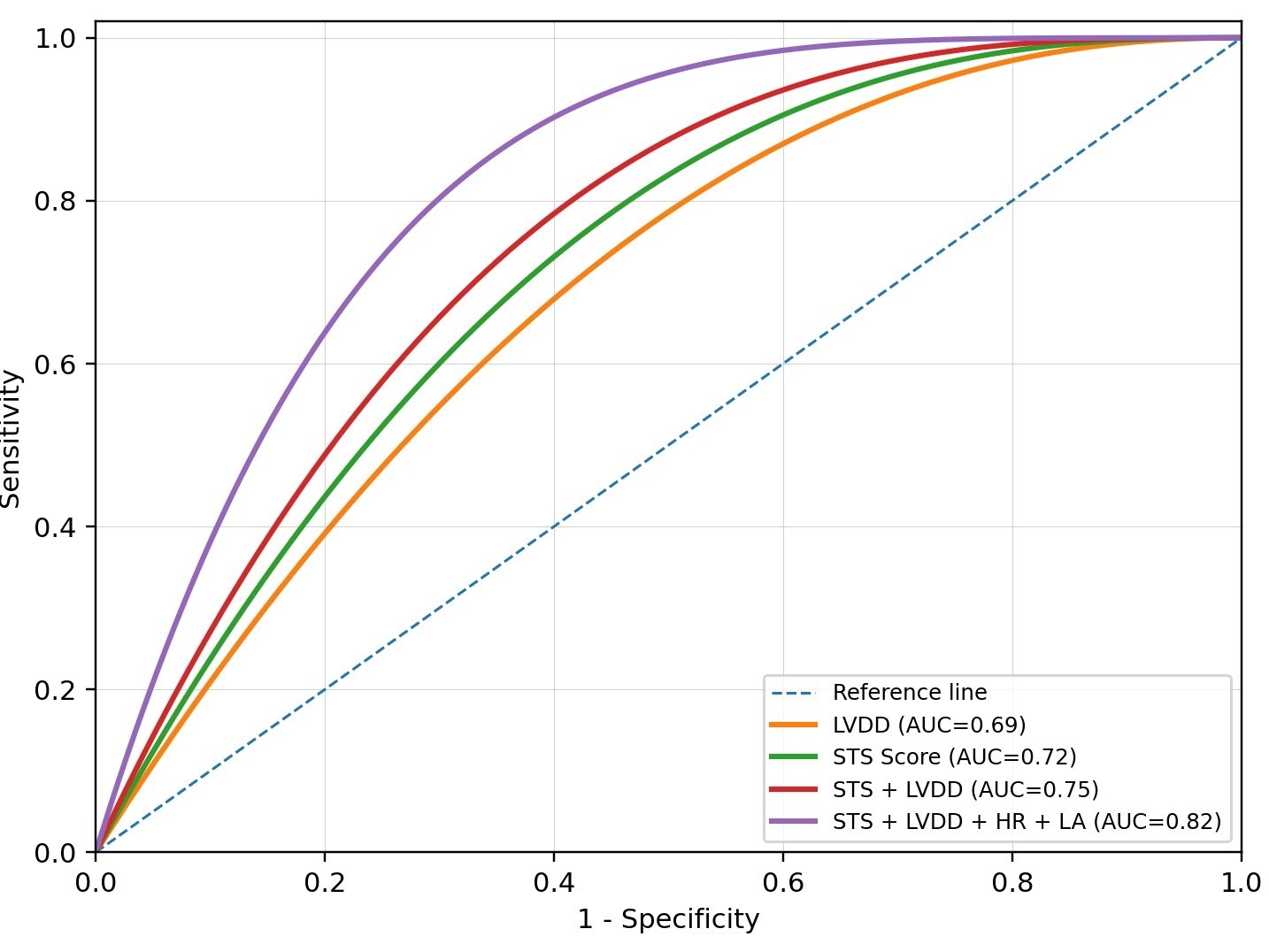
Figure 1. ROC curves of prognostic models for early postoperative complications after CABG
HR – heart rate, LA – left atrial, LVDD – left ventricular diastolic dysfunction
|
Table 3. Diagnostic performance of prognostic models |
|||||
|
Model |
AUC (95% CI) |
Sensitivity (%) |
Specificity (%) |
ΔAUC vs STS |
p (DeLong) |
|
LVDD |
0.69 (0.60–0.78) |
66.7 |
62.2 |
— |
— |
|
STS Score |
0.72 (0.64–0.80) |
68.1 |
76.5 |
— |
— |
|
STS + LVDD |
0.75 (0.68–0.83) |
76.2 |
73.5 |
+0.03 |
0.041 |
|
STS + LVDD + HR + LA |
0.82 (0.75–0.88) |
81.0 |
76.5 |
+0.10 |
<0.001 |
|
ΔAUC was calculated relative to the baseline STS Score model. p values were calculated using the DeLong method |
|||||
Discussion
The present study showed that adding echocardiographic and functional markers to the STS score improves prediction of early postoperative complications after elective CABG. The baseline STS score demonstrated moderate discrimination. The addition of LVDD provided a statistically significant improvement, and the highest prognostic accuracy was achieved by the combined model including STS score, LVDD, HR, and LA size. Because LVDD is not a single measurement but a multiparametric echocardiographic diagnosis, the present study used an operational definition based on transmitral flow, tissue Doppler indices, E/e′ ratio, TR velocity, and LA size/volume. This clarification is important because abnormal relaxation and increased filling pressure may influence the postoperative course through different mechanisms.
Isolated abnormal relaxation may indicate reduced active myocardial relaxation and early impairment of diastolic reserve, whereas elevated filling pressure and LA enlargement may reflect more advanced diastolic dysfunction, chronically increased LV filling pressures, and reduced compliance. In the perioperative setting, the latter phenotype may be particularly vulnerable to volume shifts, ischemia-reperfusion injury, systemic inflammation, tachycardia, and increased afterload. Thus, the prognostic effect of LVDD after CABG is biologically plausible and may reflect both impaired relaxation and increased filling-pressure burden. Our previous studies have shown that LVDD is an independent prognostic predictor of complications after CABG surgery (20, 21).
The observed association between LVDD and postoperative complications is consistent with the results of Metkus et al. (22), who demonstrated that preoperative diastolic dysfunction was associated with adverse outcomes after cardiac surgery, including mortality, prolonged mechanical ventilation, and longer hospitalization. Our findings further suggest that even when a validated risk model such as the STS score is used, the assessment of LVDD can provide additional prognostic information.
The inclusion of HR and LA size in the best-performing model also has clinical rationale. Increased HR shortens diastolic filling time and may aggravate impaired relaxation, especially in patients with CAD and limited myocardial reserve. LA enlargement reflects chronic exposure to elevated filling pressures and may serve as a structural marker of the cumulative burden of diastolic dysfunction. The combined model therefore integrates surgical risk, current functional status, and chronic remodeling.
Because the available sample size did not allow stable grade-specific analysis of LVDD, the primary model used LVDD as a binary variable. This approach reduces the risk of overfitting, but it may also underestimate the prognostic gradient between grade I impaired relaxation, grade II pseudonormal filling, and grade III restrictive filling. Future studies with larger samples should evaluate whether LVDD grade provides incremental value beyond binary LVDD status.
Study limitations
The study has several limitations. First, it was performed in a single center and included a relatively limited sample size. Second, postoperative complications were analyzed as a composite endpoint; individual complication categories may have different mechanisms and predictors. Third, although LVDD was defined using a multiparametric echocardiographic approach, complete grade-specific diastolic data were not uniformly available in all patients, and the main prognostic analysis therefore used a binary LVDD variable. Fourth, inter-operator variability in echocardiographic assessment cannot be fully excluded. Finally, external validation in larger multicenter cohorts is required before the model can be recommended for routine clinical implementation.
Conclusion
LVDD reflects reduced diastolic reserve and increased vulnerability to perioperative hemodynamic stress, which are not fully captured by traditional risk scores. The addition of LVDD to the STS score provides a clinically and statistically significant improvement in predicting early postoperative complications after CABG. The highest prognostic accuracy is achieved using a combined model that includes STS score, LVDD, HR, and LA size. The revised operational definition of LVDD emphasizes its multiparametric nature and recognizes the potential difference between impaired relaxation and elevated filling pressure. This strengthens the clinical interpretation of the model and supports the use of preoperative diastolic assessment for risk stratification in patients referred for elective CABG.
Ethics: The study was conducted in accordance with the ethical principles of the Declaration of Helsinki, including the 2024 revision, and with local institutional requirements for clinical research involving human participants. The study protocol was approved by Ethics Committee of Adam University N5, September 10, 2021. Informed consent was obtained from patients for diagnostic procedures, treatment, and surgery.
Peer-review: External and internal
Conflict of interest: None to declare
Authorship: A. K. N., T.Z. K, I.K. M., and A.A.S. equally contributed to the study and preparation of manuscript, its revision and all approved manuscript for publication. Thus, all authors fulfilled authorship criteria
Acknowledgements and funding: None to declare
Statement on A.I.-assisted technologies use: During the preparation of this manuscript, the authors used an AI-assisted language tool only for language editing, translation support, and improvement of clarity and structure. The authors reviewed and edited all AI-assisted output and take full responsibility for the final content, accuracy, interpretation of results, and conclusions of the manuscript.
Data and material availability: The datasets generated and analyzed during the current study are not publicly available due to institutional and patient confidentiality restrictions. De-identified data may be made available from the corresponding author upon reasonable request and with permission of the participating institution. Any share should be in frame of fair use with acknowledgement of source and / or collaboration
References
| 1.Vujcic I, Maksimovic J, Sipetic-Grujicic S. Epidemiology of ischemic heart disease. Medicinska Istrazivanja 2025: 1-11. doi:10.5937/medi0-58650 https://doi.org/10.5937/medi0-58650 |
||||
| 2. Ogryzko EV, Ivanova MA, Odinets AV, Vankov DV, Lyutsko VV. Dynamics of morbidity and mortality from acute forms of ischemic heart disease in the Russian Federation in 2012-2017. Russian Journal of Preventive Medicine 2019; 22: 23-7. doi:10.17116/profmed20192205123 https://doi.org/10.17116/profmed20192205123 |
||||
| 3. Akchurin RS, Shiryaev AA, Vasiliev VP, Galyautdinov DM, Vlasova EE. Current trends in coronary surgery. Circulation Pathology and Cardiac Surgery 2017; 21(3 Suppl): 34-44. doi:10.21688/1681-3472-2017-3S-34-44 https://doi.org/10.21688/1681-3472-2017-3S-34-44 |
||||
| 4. Shklianka IV, Zharinov OY, Mikhaliyev KO, Epanchintseva OA, Todurov BM. Early complications after isolated coronary artery bypass grafting: predictors and perioperative drug therapy. Ukrainian J Cardiovasc Surg 2019; 2: 30-9. doi:10.30702/ujcvs/19.3505/030037-039 https://doi.org/10.30702/ujcvs/19.3505/030037-039 |
||||
| 5. Bazdyrev E, Polikutina O, Kalichenko N, Slepynina Y, Barbarash O. Cardiorespiratory postoperative complications in patients with coronary artery disease after elective coronary artery bypass grafting: association with lung function. Circulation Pathology and Cardiac Surgery 20172017; 21: 85-97. doi:10.21688/1681-3472-2017-2-85-97 https://doi.org/10.21688/1681-3472-2017-2-85-97 |
||||
| 6. Syrova ID, Lozhkin IS, Trubnikova OA, Artamonova AI, Portnov YM, Semenov SE, et al. Cerebrovascular complications in patients with coronary artery disease after coronary artery bypass grafting: a 5-year follow-up. Creative Cardiology 2020; 14: 313-23. doi:10.24022/1997-3187-2020-14-4-313-323 https://doi.org/10.24022/1997-3187-2020-14-4-313-323 |
||||
| 7. Druzhina O, Loskutov O, Maruniak S. Comorbidities as a risk factor for postoperative complications in patients undergoing coronary artery bypass grafting with cardiopulmonary bypass. Emerg Med 2019; 4: 122-7. doi:10.22141/2224-0586.4.99.2019.173944 https://doi.org/10.22141/2224-0586.4.99.2019.173944 |
||||
| 8. Chen JJ, Lee TH, Kuo G, Huang YT, Chen PR, Chen SW, et al. Strategies for post-cardiac surgery acute kidney injury prevention: a network meta-analysis of randomized controlled trials. Front Cardiovasc Med 2022; 9: 960581. doi:10.3389/fcvm.2022.960581 https://doi.org/10.3389/fcvm.2022.960581 PMid:36247436 PMCid:PMC9555275 |
||||
| 9. Lazar HL. Preventing postoperative surgical-site infections in cardiac surgery. JTCVS Open 2021; 6: 1-8. doi:10.1016/j.xjon.2021.04.002 https://doi.org/10.1016/j.xjon.2021.04.002 PMid:33937880 PMCid:PMC8080169 |
||||
| 10. Nashef SAM, Roques F, Sharples LD, Nilsson J, Smith C, Goldstone AR, et al. EuroSCORE II. Eur J Cardiothorac Surg 2012; 41: 734-45. doi:10.1093/ejcts/ezs043 https://doi.org/10.1093/ejcts/ezs043 PMid:22378855 PMCid:PMC11981337 |
||||
| 11. Pocock SJ, Ariti CA, McMurray JJV, Maggioni A, Køber L, Squire IB, et al. Predicting survival in heart failure: a risk score based on 39 372 patients from 30 studies. Eur Heart J 2013; 34: 1404-13. doi:10.1093/eurheartj/ehs337 https://doi.org/10.1093/eurheartj/ehs337 PMid:23095984 |
||||
| 12. Shahian DM, O'Brien SM, Filardo G, Ferraris VA, Haan CK, Rich JB, et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 1-coronary artery bypass grafting surgery. Ann Thorac Surg 2009; 88(1 Suppl). doi:10.1016/j.athoracsur.2009.05.053 https://doi.org/10.1016/j.athoracsur.2009.05.053 PMid:19559822 |
||||
| 13. Gogaeva O. Comparison of EuroSCORE I, EuroSCORE II and STS in cardiac surgery in high-risk patients with complicated coronary artery disease. Ukrainian J Cardiovasc Surg 2020; 3: 15-21. doi:10.30702/ujcvs/20.4009/037015-021 https://doi.org/10.30702/ujcvs/20.4009/037015-021/6.89 |
||||
| 14. Mastroiacovo G, Bonomi A, Ludergnani M, Franchi M, Maragna R, Pirola S, et al. Is EuroSCORE II still a reliable predictor for cardiac surgery mortality in 2022? Eur J Cardiothorac Surg 2023; 64. doi:10.1093/ejcts/ezad294 https://doi.org/10.1093/ejcts/ezad294 PMid:37669150 PMCid:PMC10722878 |
||||
| 15. Goncharov M, Mejia OAV, Perez de Souza Arthur C, Orlandi BMM, Sousa A, Praça Oliveira MA, et al. Mortality risk prediction in high-risk patients undergoing coronary artery bypass grafting: are traditional risk scores accurate? PLoS One 2021; 16. doi:10.1371/journal.pone.0255662 https://doi.org/10.1371/journal.pone.0255662 PMid:34343224 PMCid:PMC8330943 |
||||
| 16. Torbas O. Diastolic function of the left ventricle in clinical practice. Hypertension 2021; 5-6: 5-18. doi:10.22141/2224-1485.5-6.66-67.2019.186043 https://doi.org/10.22141/2224-1485.5-6.66-67.2019.186043 |
||||
| 17. Titova AL, Saiganov SA. Left ventricular diastolic function in patients with coronary artery disease undergoing coronary artery bypass grafting. Russ Fam Physician 2014; 18: 10-7. | ||||
| 18. Nagueh SF, Sanborn DY, Oh JK, Anderson B, Billick K, Derumeaux G, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography and for heart failure with preserved ejection fraction diagnosis: an update from the American Society of Echocardiography. J Am Soc Echocardiogr 2025; 38: 537-69. doi:10.1016/j.echo.2025.03.011 https://doi.org/10.1016/j.echo.2025.03.011 PMid:40617625 |
||||
| 19. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated ROC curves: a nonparametric approach. Biometrics 1988; 44: 837-45. https://doi.org/10.2307/2531595 |
||||
| 20. Moldotashev IK, Osmonov DA, Kudaibergenova NT, Nazarov AK, Unal M, Sorokin AA. Echocardiographic predictors of the early postoperative period in patients after coronary artery bypass graft surgery. Wiad Lek 2021; 74: 395-8. doi:10.36740/WLek202103103 https://doi.org/10.36740/WLek202103103 PMid:33813439 |
||||
| 21. Osmonov D, Nazarov A, Unal M, Moldotashev I, Usubaliev N, Sorokin A, et al. Evaluation of complications predictors in the performance of coronary artery bypass grafting surgery in the cardiac surgery clinic "Bicard". Cor Vasa 2023; 65: 45-9. doi:10.33678/cor.2022.049 https://doi.org/10.33678/cor.2022.049 |
||||
| 22. Metkus TS Jr, Suarez-Pierre A, Crawford TC, Lawton JS, Goeddel L, Dodd-o J, et al. Diastolic dysfunction is common and predicts outcome after cardiac surgery. J Cardiothorac Surg 2018; 13: 67. doi:10.1186/s13019-018-0744-3 https://doi.org/10.1186/s13019-018-0744-3 PMid:29903030 PMCid:PMC6003153 |
||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
