New ESC guidelines on hypertension: key messages
EDITORIALS
New ESC guidelines on hypertension: key messages
Article Summary
- DOI: 10.24969/hvt.2017.524
- CARDIOVASCULAR DISEASES
- Published: 30/10/2024
- Received: 23/10/2024
- Accepted: 26/10/2024
- Views: 42261
- Downloads: 3099
- Keywords: blood pressure, hypertension, classification, diagnosis, treatment, guidelines
Address for Correspondence: Zhenisgul Tlegenova, Department of Internal Diseases 2, West Kazakhstan Marat Ospanov Medical University, 68, Maresyev Street, 030019, Aktobe, Kazakhstan.
Email: zhenisgul.tlegenova@zkmu.kz Mobile: +7 707 4998565
ORCID: Vadim Medovchshikov – 0000-0001-5996-8305, Zhenisgul Tlegenova - – 0000-0002-3707-7365, Nurlan Yeshniyazov – 0000-0002-5389-754X
New ESC guidelines on hypertension: key messages
Vadim Medovchshikov, Zhenisgul Tlegenova*, Nurlan Yeshniyazov
Department of Internal Diseases 2, West Kazakhstan Marat Ospanov Medical University, Aktobe, Kazakhstan
Graphical abstract
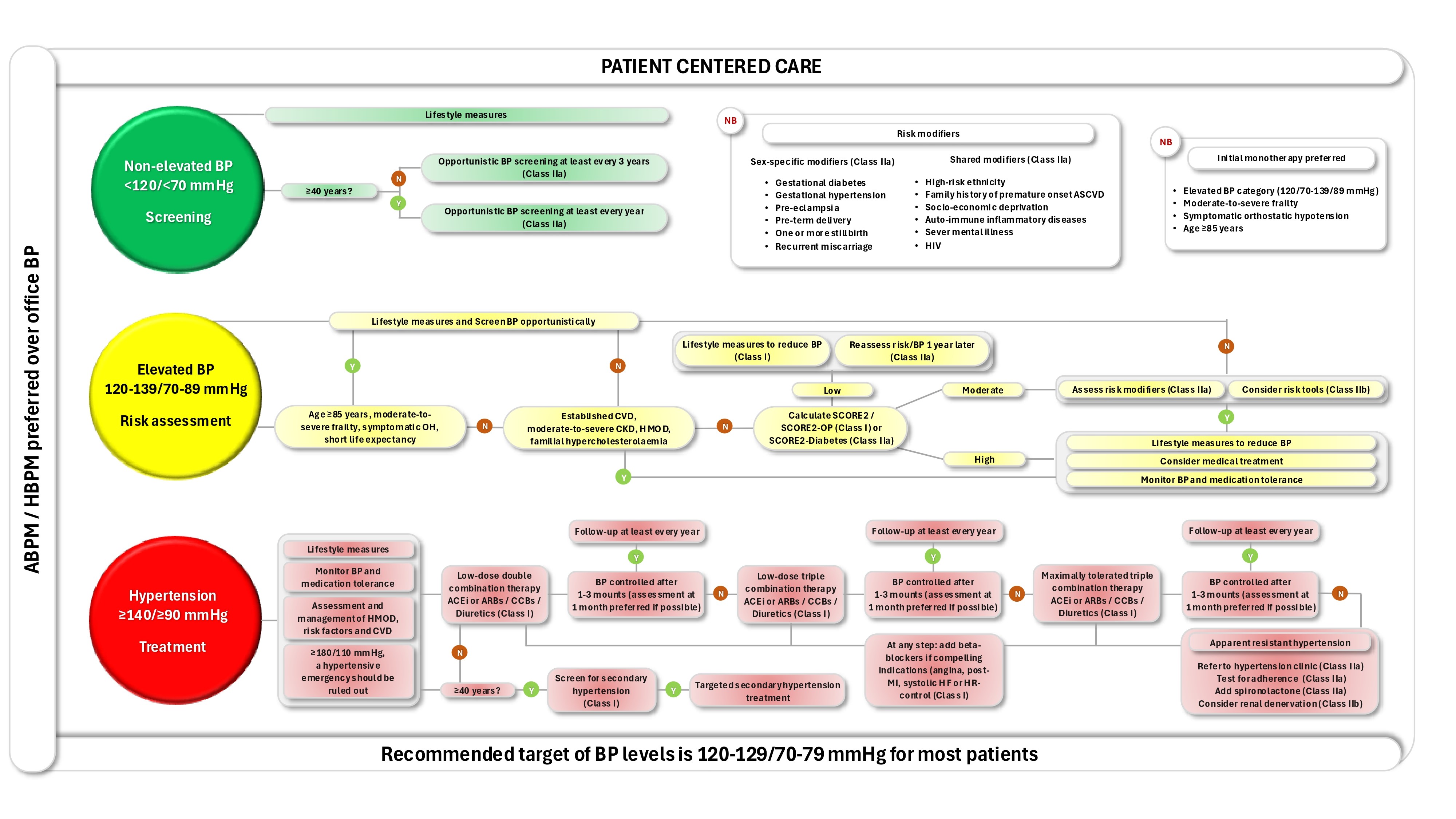
(modified from reference 1)
ABPM – Ambulatory blood pressure
monitoring; ACEi – Angiotensin-converting enzyme inhibitors; ARBs – Angiotensin receptor
blockers; BP – Blood pressure; CCBs – Calcium channel blockers; CKD – Chronic kidney disease;
CVD – Cardiovascular diseases; HBPM – Home blood pressure monitoring; HIV – Human
immunodeficiency virus; HMOD – Hypertension-mediated organ damage; OH – Orthostatic
Key words: blood pressure, hypertension, classification, diagnosis, treatment, guidelines
The hypertension guidelines, presented at the ESC Congress in London, have been given a new title: “2024 ESC Guidelines for the Management of Elevated Blood Pressure and Hypertension” (1). The discontinuation of the term “arterial” is due to a terminological clarification, as the term “arterial hypertension” may also refer to pulmonary hypertension.
![]() One of the key changes is the updated classification of blood pressure (BP): non-elevated BP (<120/70 mmHg), elevated BP (120-139/70-89 mmHg), and hypertension (≥140/90 mmHg) (1). These updates reflect an effort to harmonize approaches to the diagnosis and treatment of hypertension on a global scale. The introduction of the term “elevated BP” is not new to cardiologists. In 2017, the American College of Cardiology and the American Heart Association introduced the concept of “elevated BP” for levels of 120-129/<80 mmHg in their Guidelines, with BP levels of 130-139/80-89 mmHg classified as stage 1 hypertension (2).
One of the key changes is the updated classification of blood pressure (BP): non-elevated BP (<120/70 mmHg), elevated BP (120-139/70-89 mmHg), and hypertension (≥140/90 mmHg) (1). These updates reflect an effort to harmonize approaches to the diagnosis and treatment of hypertension on a global scale. The introduction of the term “elevated BP” is not new to cardiologists. In 2017, the American College of Cardiology and the American Heart Association introduced the concept of “elevated BP” for levels of 120-129/<80 mmHg in their Guidelines, with BP levels of 130-139/80-89 mmHg classified as stage 1 hypertension (2).
It has been convincingly demonstrated that the risk of cardiovascular (CV) events increases linearly from normotension to hypertension, but the benefits of antihypertensive treatment aimed at lowering BP are not seen in all patient groups. However, in patients with BP levels of 120-139/70-89 mmHg and elevated CV risk, antihypertensive therapy may be effective in reducing CV events and mortality (Graphical abstract), which justifies the identification of a subgroup of patients with elevated BP (1).
Another significant change is the shift of focus toward ambulatory and home blood pressure monitoring (ABPM/HBPM) as the primary methods for BP assessment and hypertension diagnosis, rather than office-based measurements. Office BP measurement is recommended for diagnosing elevated BP conditions only when ABPM or HBPM are not feasible. The predominance of ABPM and HBPM in screening and diagnosis is primarily due to growing evidence of their stronger association with clinical outcomes, their ability to detect white-coat and masked hypertension, and the lower specificity of office BP measurements for identifying hypertension (1).
In hypertension screening, for office BP of 140-159/90-99 mmHg, as well as for elevated BP with high CV risk, out-of-office BP assessment is recommended to confirm the diagnosis, followed by treatment initiation once the diagnosis is confirmed. For office BP of 160-179/100-109 mmHg, it is advised to confirm the diagnosis within one month using both office and out-of-office BP measurements to minimize treatment delay. In cases of office BP ≥180/110 mmHg, a hypertensive emergency should be ruled out. If a hypertensive emergency is diagnosed, immediate treatment is recommended. If not, the diagnosis should be confirmed and treatment initiated within a maximum of one week (1).
Compared to the 2018 Guidelines, the new version has removed the degrees and stages of hypertension, as well as several risk factors, such as hyperuricemia and elevated heart rate (HR) (3). The rationale for eliminating degrees and stages lies in the lack of evidence regarding their fundamental impact on management strategies, while the removal of certain risk factors is due to the absence of proven therapeutic benefits from targeting their control. Instead, for decisions on initiating and intensifying therapy, including the treatment of comorbid conditions (e.g., dyslipidemia), the evaluation of high-risk factors and the use of the SCORE2, SCORE2-OP, and SCORE2-Diabetes scales are recommended. In cases of borderline increased risk (5 %-< 10%), the new concept of risk modifiers – non-traditional cardiovascular diseases (CVD) risk modifiers, including gender-specific ones has been proposed. This approach ultimately allows for the initiation of pharmacological therapy for elevated BP under certain conditions (Graphical abstract) (1).
The assessment of hypertension-mediated organ damage (HMOD) has been expanded and refined. In addition to the traditional evaluation of chronic kidney disease, left ventricular (LV) hypertrophy, and arterial damage, new echocardiographic markers of LV diastolic dysfunction have been identified as independent indicators for the first time. These include a left atrial volume index >34 ml/m², left atrial volume/height² in men >18.5 ml/m² and in women >16.5 ml/m², e' <7 cm/s, and E/e' >14 (1). The inclusion of LV diastolic dysfunction as HMOD is based on its association with increased morbidity and mortality, as well as the risk of developing heart failure (HF), particularly with preserved ejection fraction (EF) (4).
For the first time, the interpretation of biomarkers of myocardial injury and stress has been introduced, including elevations in high-sensitivity troponins T or I above the 99th percentile and NT-proBNP levels of ≥125 pg/mL in individuals under 75 years and ≥450 pg/mL in those aged 75 years or older (1). Elevated levels of high-sensitivity troponins are associated with the risk of developing hypertension, LV hypertrophy, and serve as markers of increased mortality in hypertensive emergencies (5). Elevated NT-proBNP levels are found in more than a quarter of patients with hypertension and are associated with an increased risk of CVD, including HF, as well as CV and all-cause mortality (6).
The assessment of HMOD is crucial for initiating or intensifying antihypertensive therapy in patients with elevated BP and a SCORE2/SCORE2-OP risk of 5%-<10%, for the differential diagnosis of masked or white-coat hypertension, in the presence of non-traditional risk factors, in young patients (<40 years) with elevated BP, and for addressing therapeutic inertia on the part of both the physician and the patient (1).
The role of fundoscopy in diagnosing hypertensive retinopathy in patients with elevated BP and hypertension has been somewhat downgraded (IIb/B). Several trials have shown conflicting results regarding the association of mild or moderate hypertensive retinopathy with worsened prognosis, and a meta-analysis indicated only a slight increase in the risk of CVD (8).
However, fundoscopy is still recommended for all patients with BP ≥180/110 mmHg during hypertensive emergencies and malignant hypertension, as well as for patients with diabetes to rule out hemorrhages, exudates, and papilledema (1).
The treatment algorithm for hypertension has undergone changes. The document introduces new recommendations for lifestyle modifications to lower BP, including updates on physical activity and the potential use of potassium supplements. A unified and simplified initial treatment strategy is recommended for all patients, with few exceptions. This strategy involves combining two medications, and if BP is not controlled within 1-3 months, three medications at low doses, regardless of baseline BP levels or comorbid conditions (Graphical abstract). Angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, dihydropyridine calcium channel blockers, and thiazide/thiazide-like diuretics are first-line medications for effective BP reduction and, importantly, for the prevention of CV events. As a result, the focus on clinical outcomes is more explicit in the new guidelines (1).
Beta-blockers (BBs) are recommended to be added in combination with any of the aforementioned drugs when indicated, such as in cases of angina, a history of myocardial infarction, HF with reduced LV systolic function, or for HR control, for example, in atrial fibrillation (Graphical abstract). This recommendation regarding BBs is based on evidence suggesting that they are less effective in preventing HMOD and CV events, particularly stroke, and are associated with an increased risk of developing diabetes, especially when used in combination with diuretics (1).
Initial monotherapy is recommended for patients aged ≥85 years, those with symptomatic orthostatic hypotension, moderate-to-severe frailty, or elevated BP with indications for pharmacological treatment (Graphical abstract) (1).
For patients undergoing treatment, fixed combinations of two or three medications are preferred (IB). The use of fixed-dose combinations in a single pill may lead to faster and more pronounced BP reduction, reduce pill burden, and improve adherence. However, data on the impact of fixed-dose combinations on clinical outcomes are lacking. Another key limitation of prescribing fixed combinations is that they cannot be used as initial therapy due to the lack of clinical trials evaluating their safety and efficacy at treatment initiation (1).
This gap in evidence has been addressed by the GMRx2 and VERONICA-Nigeria trials, which tested fixed combinations of three drugs (telmisartan, amlodipine, and indapamide), and the QUADRO trial, which tested a fixed combination of four drugs (perindopril, indapamide, amlodipine, and bisoprolol). These trials were presented at the Hot Line 2 session of the ESC Congress in London. They have not been included in the Guidelines. All trials demonstrated the superiority of fixed combinations over standard therapy (separate tablets), including as initial therapy, and were found to be safe (VERONICA-Nigeria and QUADRO remain unpublished) (9). Additionally, polypills, which combine antihypertensive agents, lipid-lowering medications, and, when indicated, aspirin, have proven effective for the overall prevention of CVD (1).
A new BP target of 120-129/70-79 mmHg, if tolerated, has been established for most patients with elevated BP and hypertension, regardless of comorbidities. When assessing the achievement of target BP, preference should be given to out-of-office measurements (1). This more stringent target is based on key trials, including Cardio-Sis (10), SPS3 (11), SPRINT (12), and STEP (13), which investigated the effects of intensive BP control versus standard control, showing positive results in reducing the incidence of major CV events, including in elderly populations (60-80 years) (13) and those with lacunar stroke (11). The meta-analysis of 51 trials demonstrated that intensive BP control is more effective in preventing major CV events, even in older adults up to the age of 85 (14). Less strict BP targets (preferably <140/90 mmHg) should be selected for patients who cannot tolerate BP levels of 120-129/70-79 mmHg, those aged ≥85 years, individuals with symptomatic orthostatic hypotension, moderate-to-severe frailty at any age, or an expected life expectancy of less than 3 years (1).
In cases of definitively diagnosed resistant hypertension, one notable new recommendation is the option of using eplerenone in patient’s intolerant to spironolactone, as well as the consideration of renal artery denervation (IIb) in specialized centers for BP control (Graphical abstract). The main limitations preventing the widespread adoption of renal artery denervation include: (i) a potentially insufficient therapeutic effect of the procedure, comparable to the addition of a single antihypertensive medication, (ii) uncertain cost-effectiveness, and (iii) insufficient data on its long-term impact on prognosis and the development of distant complications (1).
The key evidence gaps remain as follows: (i) the impact of gender-specific risk factors on pathophysiology, outcomes, and potential adjustments in antihypertensive therapy; (ii) validation of new devices for BP measurement; (iii) the potential benefits of treating elevated BP in low-risk patients; (iv) CV outcomes of treating elevated BP and hypertension in young (<40 years) and elderly (≥85 years) patients, as well as those with symptomatic orthostatic hypotension or moderate-to-severe frailty at any age; (v) the management of hypertension and prevention of events in patients undergoing cancer treatment or following transplantation; (vi) the potential antihypertensive effects of sacubitril/valsartan, SGLT2 inhibitors, GLP-1 receptor agonists, and finerenone (1).
At the same time, the medical community holds high expectations for the fundamentally new and innovative medications currently being studied for the treatment of hypertension: aldosterone synthase inhibitors (Baxdrostat, Lorundrostat, BI 690517), dual endothelin-A and -B receptor antagonists (Aprocitentan), small interfering RNA that suppresses hepatic angiotensinogen expression (Zilebesiran), and hepatocyte-directed antisense oligonucleotide targeted to angiotensinogen mRNA (Evazarsen sodium).
In summary, the new guidelines emphasize a patient-centered approach to managing individuals with elevated BP and hypertension. Collaboration among healthcare professionals across different levels and specialties, as well as with patients, is essential for successfully reducing the burden of conditions associated with elevated BP and hypertension.
Peer-review: Internal
Conflict of interest: None to declare
Authorship: V.M., Zh.T. and N.Y. equally contributed to manuscript preparation and fulfilled the authorship criteria.
Acknowledgement and Funding: None to declare
Statement on A.I.-assisted technologies use: Authors declared they did not use A.I.- assisted technologies in preparation of manuscript
Availability of data and material: Not applied
References
| 1.McEvoy JW, McCArthy CP, Bruno RM, Brouwers S, Canavan MD, Ceconi C, et al. 2024 ESC Guidelines for the management of elevated blood pressure and hypertension. Eur Heart J. 2024:ehae178. doi: 10.1093/eurheartj/ehae178 https://doi.org/10.1093/eurheartj/ehae178 |
||||
| 2.Whelton PK, Carey RM, Aronov WS, Casey DE, Collins KJ, Dennison Himmefarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018; 71: 1269-324. doi: 10.1161/HYP.0000000000000066 https://doi.org/10.1161/HYP.0000000000000066 |
||||
| 3.Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J 2018; 39: 3021-104. doi: 10.1093/eurheartj/ehy339 https://doi.org/10.1093/eurheartj/ehy339 |
||||
| 4.Ottosen CI, Nadruz W, Inciardi RM, Johansen ND, Fudim M, Biering T, et al. Diastolic Dysfunction in Hypertension: A Comprehensive Review of Pathophysiology, Diagnosis, and Treatment. Eur Heart J Cardiovasc Imaging 2024: jeae178. doi: 10.1093/ehjci/jeae178. https://doi.org/10.1093/ehjci/jeae178 |
||||
| 5.McEvoy JW, Chen Y, Nambi V, Ballantyne CM, Sharrett AR, Appel LJ, et al. High-sensitivity cardiac troponin T and risk of hypertension. Circulation 2015; 132: 825-33. doi: 10.1161/CIRCULATIONAHA.114.014364 https://doi.org/10.1161/CIRCULATIONAHA.114.014364 |
||||
| 6.Daya NR, McEvoy JW, Christenson RH, Tang O, Foti K, Juraschek SP, et al. Prevalence of elevated NT-proBNP and its prognostic value by blood pressure treatment and control. Am J Hypertens 2023; 36: 602-11. doi: 10.1093/ajh/hpad065 https://doi.org/10.1093/ajh/hpad065 |
||||
| 7.Kim W, Kim BS, Kim HJ, Lee JH, Shin J, Shin JH. Clinical implications of cardiac troponin-I in patients with hypertensive crisis visiting the emergency department. Ann Med 2022; 54: 507-15 doi: 10.1080/07853890.2022.2034934 https://doi.org/10.1080/07853890.2022.2034934 |
||||
| 8.Liew G, Xie J, Nguen H, Keay L, Kamran Ikram M, McGeechan K, et al. Hypertensive retinopathy and cardiovascular disease risk: 6 population-based cohorts meta-analysis. Int J Cardiol Cardiovasc Risk Prev 2023;17:200180 doi: 10.1016/j.ijcrp.2023.200180 https://doi.org/10.1016/j.ijcrp.2023.200180 |
||||
| 9.Rodgers A, Salam A, Schutte AE, Cushman WC, Asita de Silva H, Di Tanna CL, et al. Efficacy and safety of a novel low-dose triple single-pill combination compared with placebo for initial treatment of hypertension. J Am Coll Cardiol 2024: S0735-1097(24)08227-5. doi: 10.1016/j.jacc.2024.08.025 https://doi.org/10.1016/j.jacc.2024.08.025 |
||||
| 10.Verdecchia P, Staessen JA, Angelli F, de Simone G, Achilli A, Ganau A, et al. Usual versus tight control of systolic blood pressure in non-diabetic patients with hypertension (Cardio-Sis): an open-label randomized trial. Lancet 2009; 374: 525-33. doi: 10.1016/S0140-6736(09)61340-4 https://doi.org/10.1016/S0140-6736(09)61340-4 |
||||
| 11.Benavente OR, Coffey CS, Conwit R, Hart RG, McClure RA, Pearce LA, et al. Blood-pressure targets in patients with recent lacunar stroke: the SPS3 randomized trial. Lancet 2013; 382: 507-15. doi: 10.1016/S0140-6736(13)60852-1 https://doi.org/10.1016/S0140-6736(13)60852-1 |
||||
| 12.Wright JT Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, Rocco MV, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 2015; 373: 2103-16. doi: 10.1056/NEJMoa1511939 https://doi.org/10.1056/NEJMoa1511939 |
||||
| 13.Zhang W, Zhang S, Deng Y, Wu S, Ren J, Sun G, et al. Trial of intensive blood-pressure control in older patients with hypertension. N Engl J Med 2021; 385: 1268-79. doi: 10.1056/NEJMoa2111437 https://doi.org/10.1056/NEJMoa2111437 |
||||
| 14.Blood Pressure Lowering Treatment Trialists' Collaboration. Age-stratified and blood-pressure-stratified effects of blood-pressure-lowering pharmacotherapy for the prevention of cardiovascular disease and death: an individual participant-level data meta-analysis. Lancet 2021; 398: 1053-64. doi: 10.1016/S0140-6736(21)01921-8 https://doi.org/10.1016/S0140-6736(21)01921-8 |
||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
