Conflict resolution style in professional activities of nurses
ORIGINAL RESEARCH ARTICLE
Conflict resolution style in professional activities of nurses
Article Summary
- DOI: 10.24969/hvt.2024.544
- CARDIOVASCULAR DISEASES
- Published: 04/02/2025
- Received: 11/09/2024
- Revised: 09/01/2025
- Accepted: 10/01/2025
- Views: 17053
- Downloads: 4765
- Keywords: Conflicts, causes of conflict, conflict resolution, conflict style, nurse
Address for Correspondence: Aigul S. Abdyzhalieva, Kyrgyz State Medical Institute of Post-Graduate Training and Continuous Education named after S.B. Daniyarov, Bishkek, Kyrgyzstan
E-mail: a.abdyjalieva77@gmail.com
ORCID: Aigul S. Abdyzhalieva - 0009-0004-8676-7508; Victor E. Savin -0000-0001-6963-9505; Tologon Ch. Chubakov - 0000-0002-7876-5332; Kalima T. Mamatova - 0009-0000-1093-0947; Raikhan S. Rozyeva - 0009-0002-8009-6147
Facebook: Aigul S. Abdyzhalieva A. S –- aigul.abdyjalieva; Victor E. Savin - 1BLfJbETBS; Kalima T. Mamatova - 1CuCb9v7k1; Raikhan S. Rozyeva - 15U7elwH6
Twitter (X): Aigul S. Abdyzhalieva - @aigul_kgmipk Linkedin : Kalima T. MAmatova - kalima-mamatova-9349a377
Aigul S. Abdyzhalieva1*, Victor E. Savin2, Tologon Ch. Chubakov1, Kaliman T. Mamatova1, Raikhan S. Rozyeva1
1Kyrgyz State Medical Institute of Post-Graduate Training and Continuous Education named after S.B. Daniyarov, Bishkek, Kyrgyzstan
2Bishkek State University named after K. Karasaev, Bishkek, Kyrgyzstan
Abstract
Objective: To analyze the causes and styles of conflict resolution in professional activities of nurses working in medical and preventive organizations of the healthcare system.
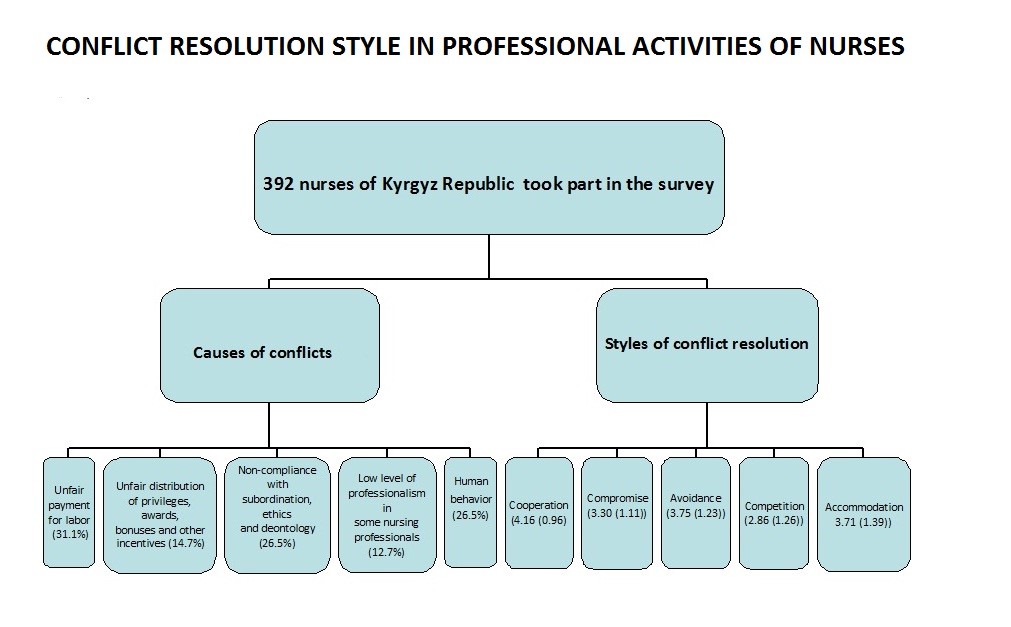
Methods: Overall, 392 nursing professionals working in medical and preventive organizations took part in the research. To address the purpose of the work, we used a questionnaire of sociodemographic characteristics and a list of different styles of organizational conflict resolution developed by Rahim Organizational Conflict Inventory (Rahim 1983).
Results: The results indicate that the most common causes of conflict among nurses are unfair pay (31.1%), lack of respect for subordination (26.5%), and human behavior (26.5%). The nurses’ preferred conflict management styles are cooperation, which scored the highest mean score of all conflict management styles (4.16 (0.96)) points, and avoidance and accommodation styles were in the second place. The mean scores of these two styles were almost at the same level (3.75 (1.23) and 3.71 (1.39)) points.
Conclusion: Conflicts in professional activities of nurses in the Kyrgyz Republic are a serious problem in medical and preventive organizations. The main styles of conflict resolution used by nurses are cooperation, avoidance and accommodation.
Key words: Conflicts, causes of conflict, conflict resolution, conflict style, nurse
Introduction
Conflict is a lack of agreement between two or more parties, which may be specific individuals or groups of individuals. Each party makes every effort to get its point of view or goal accepted and prevents the other party from making the same (1-4). Conflict arises in the life of any organization because an organization is a group of people whose activities are consciously coordinated to achieve common goals. (5-9). This type of disagreement from time to time arises in healthcare organizations, like in any other organization. Healthcare organizations play a vital role in achieving the goals of health systems and this characteristic distinguishes them from other organizations which activities are not related to public health (10-12). The complexity of the conflict structure makes recognizing and managing conflict a complex process and requires appropriate skills for professional work. The ability to understand the nature of conflicts, to differentiate their components and to work towards their resolution is an important component of the professional profile of managers of healthcare organizations and health authorities (2, 13, 14). In healthcare organizations, failure to manage conflict is a major cause of stressful work environments, physical plays, patient and staff dissatisfaction, poor quality of care and increased costs (15-17).
Graphical abstract
Kenneth Thomas - Ralph Kilmann (18, 19) identified the following ways of managing conflict: cooperation, competition, avoidance, accommodation, compromise:
1. Cooperative strategy - accepting the differences in views between the parties and the desire to understand the opponent’s point of view, discuss the reasons for the situation and find a solution that satisfies the interests of the both parties.
2. Competitive strategy - the desire to satisfy one’s personal interests while displacing other participants in a conflict situation.
3. Evasion strategy is the avoidance of solving the situation, the desire to delay the time or a complete lack of desire to solve the conflict.
4. Accommodation strategy is a muting, suppression of the conflict, satisfaction of the goals and interests of the other party, the refusal of confrontation.
5. Compromise strategy is a temporary reaching an agreement, willingness to make concessions to each other.
Nurses, being the largest group of health workers in any healthcare organization, are not immune to conflict (20-24). Conflict among nurses has been recognized as a global serious problem in healthcare organizations. It can arise as a result of several elements such as complexity in the organization, different role expectations, interdepartmental competition, constraints in decision-making process, competition for limited resources, unclear work boundaries and personality differences (10, 25- 27).
If conflict is not handled properly, it can significantly affect employee morale, increase turnover and even lead to litigation, ultimately affecting the overall wellbeing of the organization (28- 30). da Silva Ferreira et al. (31) in a recent literature review indicated that the implementation of proposed conflict prevention and management strategies in the nursing sector addresses interpersonal tensions and plays a key role in improving the organizational climate and quality of patient care. By developing the culture of open and effective communication, where nursing professionals can constructively express their concerns, healthcare organizations create a more collaborative and harmonious working environment. Prioritizing staff well-being and job satisfaction not only improves the organizational environment but also raises standards of patient care, contributing to positive health outcomes and a more humanized and positive hospital experience (31).
Objective: To analyze the causes and styles of conflict resolution in professional activities of nurses working in medical and preventive organizations of the healthcare system.
Heart, Vessels and Transplantation 2025; 9: doi: 10.24969/hvt.2025.544
![]() How nurses resolve conflicts Abdyzhalieva et al.
How nurses resolve conflicts Abdyzhalieva et al.
Methods
Our research paper was designed as a descriptive survey study. The study involved 392 nursing professionals (deputy nursing managers of healthcare organization, head nurses, senior nurses and nurses) working in healthcare organizations (public hospitals, family medicine centers, private hospitals, etc.).
All nurses provided informed consent to participate in the survey. The approval of Institutional Ethics Committee was obtained.
Baseline characteristics
We collected the following demographic, educational and professional data: age, gender, marital status, educational level, place of work, position at work, and length of service of nurses (see below).
Questionnaire
We used a questionnaire of sociodemographic characteristics and the Organizational Conflict Inventory developed by Rahim Organizational Conflict Inventory (19). The questionnaire presented by us additionally included 13 items that asked about age, gender, marital status, educational level, length of service of nurses and the main causes of conflict situations in healthcare organizations. In the questionnaire, the participants did not choose one cause of conflict but all causes of conflict that they encounter in their professional activities.
The second questionnaire includes 34 items defining conflict resolution styles. It should be noted that we reduced the number of items in the questionnaire recommended by Rahim (32) by one item due to the same content of the questions asked: item 9 was removed because item 20 contains approximately the same question. The magnitude of the indicators of different conflict resolution styles was determined on a 5-point Likert scale. The items of the questionnaire were rated as following: 1 - never, 2 - rarely, 3 - sometimes, 4 - frequently, 5 - constantly. The questionnaire contains five subscales: cooperation (items 1,4,6,14,27,28,34), avoidance (items 3,7,21,22,31,32,33), competition (items 8,9,10,17,23,26,30), accommodation (items 2,11,12,15,16,24,29), compromise (items 5,13,18,19,20,25) (Appendix 1). To analyze the scales, the mean scores obtained on each of the subscale are considered. Of all the subscales, the one with the highest mean score is considered to be the preferred style of conflict management and resolution (19, 32-34).
Statistical analysis
Statistical analysis of the obtained data was performed using SPSS 16.0. with calculation of arithmetic mean (M), standard deviation (δ), mean error of arithmetic mean (m), reliability coefficient (Student’s t-test). Differences were considered statistically significant at p < 0.05.
Results
Out of 392 participants, 387 (98.7%), were women, 5 (1.2%) were men, 320 (81.6%) were working in a public hospital, 55 (14.0%) in a family medicine center, 17 (4.3%) in other institutions. The category of nursing specialists is represented as follows: the share of practicing nurses was 61.4%, senior nurses - 31.6%, head nurses - 5.6%, deputy heads of healthcare organization in nursing - 1.2% (Table 1).
Table 2 presents the main causes of conflicts in the professional activities of nursing specialists. The most frequent causes of conflicts in nurses are unfair pay (31.1%), non-compliance with subordination, ethics and deontology (26.5%), human behavior (26.5%) and unfair distribution of privileges, awards, bonuses and other incentives (14.7%) and low level of professionalism in some nursing professionals (12.7%).
The causes of conflicts that scored the lowest were improper work organization (5.1%), striving for position and fighting for position (1.2%) and ineffective communication (3.3%). The share of these causes of conflicts in other authors’ studies was relatively low (31, 35).
We analyzed the ways of conflict resolution by nursing professionals in their professional activities (cooperation, competition, avoidance, accommodation, compromise). Table 3 presents the average assessments of the types of conflict resolution in the activities of nurses.
As can be seen from Table 3, the nurses’ preferred conflict management style is the cooperation style, which scored the highest mean score of all conflict management styles (4.16 (0.96)) points, while the avoidance and accommodation styles took the second place. The mean scores of these two styles were almost at the same level (3.75 (1.23) and 3.71 (1.39)) points. Compromise style is the fourth most preferred style by nurses (3.30 (1.11)) scores. According to our data, the style that is least frequently resorted to by nurses in conflict situations is competition (mean score - 2.86 (1.26)) points.
|
Table 1. Characteristics of indicators of nursing specialists (n=392) |
||
|
Variables |
Number of participants (n=392) |
% |
|
Sex |
|
|
|
Women |
387 |
98.7 |
|
Men |
5 |
1.2 |
|
Age, years |
|
|
|
20-25 |
22 |
5.6 |
|
26-30 |
31 |
7.9 |
|
31-40 |
81 |
20.6 |
|
41-59 |
229 |
58.4 |
|
60 and older |
29 |
7.3 |
|
Level of education |
|
|
|
Secondary specialized (medical school or college) |
372 |
94.8 |
|
Higher nursing |
16 |
4.0 |
|
Other higher education |
4 |
1.0 |
|
Institutions, place of employment |
|
|
|
State hospital, clinic (research centers and institutes) |
320 |
81.6 |
|
Family practice center |
55 |
14.0 |
|
Private hospital/clinic |
6 |
1.5 |
|
Other |
11 |
2.8 |
|
Position held |
|
|
|
Deputy heads of healthcare organizations for nursing |
5 |
1.2 |
|
Chief nurse |
22 |
5.6 |
|
Senior nurse |
124 |
31.6 |
|
Nurse |
241 |
61.4 |
|
Length of experience in position held, years |
|
|
|
1 – 5 years |
114 |
29.0 |
|
6 – 10 years |
62 |
15.8 |
|
11 years and above |
216 |
55.1 |
|
Table 2. Causes of conflicts in professional activities among nursing specialists |
||
|
Name of the causes of conflicts |
Volume ratio (n=392) |
% |
|
Unfair distribution of privileges, awards, bonuses and other incentives |
58 |
14.7 |
|
Unfair wages |
122 |
31.1 |
|
High ambitions of some employees |
48 |
12.2 |
|
Improper organization of work |
20 |
5.1 |
|
Peculiarities of behavior of managers (including abuse of authority) |
32 |
8.1 |
|
Feelings of envy among workers |
36 |
9.1 |
|
Low level of professionalism of some employees |
50 |
12.7 |
|
The desire to take a position and the struggle for a position |
5 |
1.2 |
|
Unclear distribution of responsibilities |
30 |
7.6 |
|
Ineffective communication |
13 |
3.3 |
|
Poor working conditions (lack of them) |
38 |
9.6 |
|
Failure to comply with subordination, ethics and deontology |
104 |
26.5 |
|
Human behavior |
104 |
26.5 |
|
Table 3. Average ratings of types of conflict resolution styles of nurses |
|||
|
Style |
Mean (SD) |
Min – Max |
Cronbach's alpha |
|
Collaboration |
4.16 (0.96) |
3.83 – 4.67 |
0.978 |
|
Avoidance |
3.75 (1.23) |
2.85 – 4.38 |
0.984 |
|
Competition |
2.86 (1.26) |
1.99 – 3.37 |
0.987 |
|
Accommodation |
3.71 (1.39) |
3.39 – 4.23 |
0.985 |
|
Compromise |
3.30 (1.11) |
1.99 – 3.86 |
0.972 |
Table 4 presents the results of the analysis of conflict resolution styles and compared them depending on the socio-demographic characteristics of nursing professionals. The cooperation style was resorted to men more often than the other styles by participants of all age ranges, they were competitive that women and less likely to compromise. For participants of all age ranges, the avoidance style took the second place followed by adaptation, compromise, and the last style chosen was the competition style.
|
Table 4. Comparison of average scores obtained by types of conflict resolution styles in the activities of nurses, depending on socio-demographic characteristics |
|||||
|
Variables |
Collaboration |
Avoidance |
Competition |
Accommodation |
Compromise |
|
Sex |
|||||
|
Women |
4.15±0.914 |
3.77±1.19 |
2.86±1.21 |
3.71±0.946 |
3.29±1.03 |
|
Men |
4.40±0.884 |
3.86±0.62 |
3.00±1.22 |
3.80±0.818 |
2.96±1.10 |
|
P |
0.475 |
0.711 |
0.778 |
0.885 |
0.564 |
|
Age |
|||||
|
20-25 years |
4.06±0.856 |
3.86±1.05 |
2.82±1.16 |
3.76±0.90 |
3.14±1.05 |
|
26-30 years old |
4.00±0.864 |
3.68±1.26 |
3.06±1.16 |
3.68±0.92 |
3.28±1.14 |
|
31-40 years old |
4.03±0.942 |
3.66±1.18 |
2.87±1.23 |
3.68±0.96 |
3.17±1.04 |
|
41-59 years old |
4.23±0.823 |
3.81±1.18 |
2.81±1.18 |
3.75±0.89 |
3.34±0.96 |
|
60 and older |
4.29±0.756 |
3.97±1.19 |
2.80±1.21 |
3.72±0.94 |
3.35±0.93 |
|
p |
0.452 |
0.553 |
0.685 |
0.811 |
0.603 |
|
Education |
|||||
|
Specialized secondary |
4.16±0.87 |
3.80±1.18 |
2.86±1.22 |
3.71±0.95 |
3.31±1.03 |
|
Higher nursing |
4.04±0.88 |
3.34±1.28 |
2.87±1.09 |
3.75±0.79 |
3.20±0.99 |
|
Other higher |
4.43±0.42 |
3.07±1.24 |
2.96±0.98 |
3.25±0.81 |
3.38±1.01 |
|
p |
0.521 |
0.352 |
0.904 |
0.495 |
0.777 |
|
Position |
|||||
|
Deputy heads of health care organizations for nursing |
4.29±0.94 |
3.83±1.22 |
2.86±1.52 |
3.86±1.19 |
3.30±1.01 |
|
Chief nurse |
4.21±0.87 |
3.70±1.21 |
2.81±1.20 |
3.60±0.89 |
3.33±1.02 |
|
Head nurse |
4.33±0.75 |
3.70±1.21 |
2.85±1.21 |
3.74±0.88 |
3.49±0.96 |
|
Nurse |
4.05±0.91 |
3.81±1.16 |
2.87±1.19 |
3.70±0.96 |
3.19±1.04 |
|
p |
0.134 |
0.786 |
0.914 |
0.732 |
0.575 |
|
Experience in position held |
|||||
|
15 years |
4.28±0.79 |
3.63±1.24 |
2.86±1.21 |
3.74±0.92 |
3.45±0.97 |
|
6 – 10 years |
4.18±0.89 |
3.58±1.25 |
2.93±1.27 |
3.62±0.85 |
3.49±0.99 |
|
11 years and above |
4.38±0.72 |
3.79±1.16 |
2.82±1.21 |
3.74±0.88 |
3.48±0.97 |
|
p |
0.391 |
0.239 |
0.786 |
0.711 |
0.909 |
In terms of education levels, nurses with secondary and tertiary education chose the cooperative style to a greater extent and the competitive style to a lesser extent. The second most preferred style was the avoidance style among nurses with secondary education and the accommodation style among nurses with tertiary education. Next, specialists with secondary education chose the accommodation style, then the style of compromise and competition, and specialists with tertiary education - avoidance, compromise, competition, respectively.
Our data show that regardless of the positions held, the participants are most committed to the cooperative style and least committed to competition. According to the data presented, the proportion of nurses with 10 years of professional experience and above who have chosen the cooperative style is slightly higher than employees with professional experience up to 10 years. But nevertheless, employees with 1-5 years of experience and 6-10 years of experience are also more committed to the collaborative style and they scored the lowest on the competition style.
Discussion
The most frequent causes of conflicts between nurses in our study were unfair pay, non-compliance with subordination, ethics and deontology, human behavior and unfair distribution of privileges, awards, bonuses and other incentives and low level of professionalism in some nursing professionals.
According to da Silva Ferreira R. et al. (31), the main causes of conflict among nurses were found to be work overload, poor communication, inconsistencies in the performance of professional procedures and misallocation of resources (31). Another paper reflects the same causes as in the previous article, except for conflicts related to work overload (35). It should be noted that most nurses working in intensive care units experience moderate to high levels of conflicts. Among conflicts, competitive and intra-collective conflicts were the most frequent and moderately experienced types of conflicts (36).
In contrast, according to our data, the causes of conflicts that scored the lowest were improper work organization, striving for position and fighting for position and ineffective communication. The share of these causes of conflicts in other authors’ studies was also relatively low (31, 35).
Summarizing our data on causes of conflicts, it can be noted that such reasons as unfair pay and unfair distribution of privileges, awards, bonuses and other incentives lead to conflicts between administration and nurses, while the other reasons lead to conflicts both within the team and between nurses and patients.
Analyzing the conflict resolution results, we found that when conflicts arise, nurses most often chose more favorable styles (collaboration, accommodation, avoidance and compromise), trying not to cause repeated disagreements.
According to some authors, effective conflict management strategies, such as establishing clear communication channels, ongoing conflict resolution training, creating a collaborative environment and implementing supportive professional interventions, are considered essential to mitigate conflict and promote a healthy team climate (7, 11, 31, 36, 37). It has been proven that nurse managers with higher levels of psychoemotional intelligence are more likely to use cooperation and compromise styles of conflict resolution (38). It is interesting to note that the results obtained by Demeubaeva et al. (39) showed that the most preferred style of behavior of hospital nurses in conflict conditions is accommodation, compromise, followed by withdrawal from the conflict. According to their data, in contrast to the results of studies by a number of authors, cooperation as a style of conflict resolution did not show a significant relationship. This fact requires attention, as cooperation is the best option for maintaining a benevolent and comfortable environment in a healthcare organization (39).
When we analyzed types of conflict resolutions according to sex, age, education and position level and level of experience, there were no significant differences, however following trends worth noting; male nurses were more prone to collaborate, compete and less compromise than women ones; the collaboration was characteristic for all ages, followed by avoidance, adaptation, compromise and lastly competition; nurses with secondary and tertiary education preferred to cooperate rather than to compete, nurses with secondary education also avoid conflict situations, while nurses with tertiary education chose accommodation style, and specialists with secondary indicated accommodation as first choice, followed by compromise and competition, and specialists with tertiary education - avoidance, compromise, competition, respectively; all nurses irrespectively of the position held at work and nurses with more longer experience were committed to cooperation and similarly
Study limitations
Our study has limitations as its descriptive design and a relatively small sample size for comparative analysis of conflict resolution styles according to socio-demographic and professional characteristics.
Further larger studies involving more nurses with determination of sample size necessary to prove mean difference should be addressed to determine the conflict resolution styles distribution according to socio-demographic characteristics and also study with selection of representative sample to make the results generalizable to all city or country should be pursued. It should be noted that these studies in the Kyrgyz Republic were conducted for the first time, and a comprehensive analysis and obtaining reliable results in the field of conflict resolution in nursing require further comprehensive researches.
Conclusion
The results of a sociodemographic survey of nursing professionals in a healthcare organization indicate that unfair pay, lack of ethics and deontology, unfair distribution of privileges and interpersonal reasons were found to be the main causes of conflicts in healthcare organizations. According to our data, the preferred style of conflict resolution is cooperation, followed by avoidance, accommodation, compromise and competition. Analysis of sociodemographic characteristics showed that older nurses and those with secondary and tertiary education tend to choose the cooperative style. Employees with professional experience of 10 years and more also choose the above styles. Using this style of conflict resolution, nursing professionals make every effort to find alternative and unconventional solutions.
Ethics: All nurses provided informed consent to participate in the survey. The approval of Institutional Ethics Committee was obtained
Peer-review: External and internal
Conflict of interest: None to declare
Authorship: A.S. A., V.E.S., T.Ch.Ch., K.T. M., and R.S.R. equally contributed to preparation of the manuscript and fulfilled authorship criteria
Acknowledgement and funding: None to declare
Statement on A.I.-assisted technologies use: Authors declared they did not use artificial intelligence in preparation of manuscript
Availability of data and material: Contact authors of article for collaboration queries. In case authors share data, fair use with acknowledgement of authors, data source, citation and collaboration rules apply
References
| 1.Galitskaya I.K. Conflict and stress management in the environment of nursing staff of medical and preventive organisations. Head Med Nurse 2006; 2-3; 10-5. | ||||
| 2.Skjorshammer M. Conflict management in a hospital: designing processing structures and intervention methods. Journal of Management in Medicine 2001; 15:. 156-66. https://doi.org/10.1108/02689230110394660 PMid:11547823 |
||||
| 3.Kilag OKT, Largo JM, Rabillas AR, Kilag FE, Angtud MKA, Book JFP, et al. Administrators' Conflict Management and Strategies. IMJRISE 2024; 1: 60-7. https://doi.org/10.61796/ejheaa.v1i2.98 |
||||
| 4.de Oliveira Dias M, Lafraia J, Schmitz T, Veiera P. Systematic literature review on negotiation & conflict management . Eur J Theor Appl Sci 2023; 1: 20-31. https://doi.org/10.59324/ejtas.2023.1(3).03 |
||||
| 5.Maslova SV. Conflict resolution studies. Study guides. Tomsk: TPU; 2010.pp. 72. | ||||
| 6.Thomas KW. Conflict and negotiation processes in organizations. In: Dunnette MD, Hough LM, eds. Handbook of Industrial and Organizational Psychology. Consulting Psychologists Press; Palo Alto, CA. USA: 1992. pp. 651-717, | ||||
| 7.Tuncay OF, Yaşar Ö, Sevimligül G. Conflict management styles of nurse managers working in inpatient institutions: The case of Turkey. J Nurs Manag 2018; 26: 945-52. doi: 10.1111/jonm.12609 https://doi.org/10.1111/jonm.12609 PMid:30238532 |
||||
| 8.Komarov YuV. Conflict management in collectives. Reclamation as a Driver of Agro-Industrial Complex Modernization in the Context of Climate Change. 2023. pp. 374-378. | ||||
| 9.Vientiany D. Conflict management in organizations. J Qualit Quant Res 2024; 1: pp. 200-12. https://doi.org/10.61166/interdisiplin.v1i4.42 |
||||
| 10.Patton CM. Conflict in Health Care: A Literature Review. Internet J Healthcare Admin 2014; 9: 1-11. | ||||
| 11.Djaha YTL. Conflict management strategies used by nursing executives: An integrative review. NHIHC 2024; 2: 144-55. | ||||
| 12.Abdyzhalieva AS, Mamatova KT, Rozieva RS. Foundations of conflictology in health management: conflicts and their resolution. Health Care Kyrgyzstan 2022; 4: 216-20. https://doi.org/10.51350/zdravkg2022.4.10.31.216 |
||||
| 13.Volchansky ME. Sociology of conflict in medicine. Author's Abstract. Dissertation. Doctor of Socio-Scientific Sciences. Volgograd, 2008. | ||||
| 14.Erofeev SV, Zharov VV. Conflict between a patient and a medical staff: Analysis and prevention. Medl Law 2002; 1; 22-4. | ||||
| 15.Kantek F, Kavla I. Nurse-nurse manager conflict: How Do nurse managers manage it? Health Care Man 2007; 26: 147-51. https://doi.org/10.1097/01.HCM.0000268618.33491.84 PMid:17464228 |
||||
| 16.Whitehead DK, Weiss SA, Tappen RM. Essentials of nursing leadership and management. 4th ed. F.A. Davis Company; PA: 2007. | ||||
| 17.Al Kiyumi M. H. Conflict management in healthcare leadership; A narrative review. J Med Health 2023; 251: 2-9. DOI: doi. org/10.47363/JMHC/2023 | ||||
| 18.Kilmann RH, Thomas KW. Developing a forced-choice measure of conflict-handling behavior: The "MODE" instrument. Educ Psychol Meas1977; 37: 309-25. https://doi.org/10.1177/001316447703700204 |
||||
| 19.Rahim MA. Managing conflict in organizations. Routledge, 2023. https://doi.org/10.4324/9781003285861 |
||||
| 20.Higazee MZA. Types and levels of conflicts experienced by nurses in the hospital settings. Health SciJ 2015;, 9: 1-6. | ||||
| 21.Burns N, Grove SK. The practice of nursing research: Conduct, critique and utilization. WB Saunders, Philadelphia, PA: 1997. pp. 426-435. | ||||
| 22.McKibben, L. Conflict management: importance and implications. Br J Nurs 2017; 26: 100-3. https://doi.org/10.12968/bjon.2017.26.2.100 PMid:28132555 |
||||
| 23.Hussain N, Kousar R, Asif M, Bibi S. Conflict resolution styles among nursing staff public sector hospital-a crossover study. Ann Punjab Med Coll 2023; 17: 50-3. | ||||
| 24.Liu Y, et al. Ethical conflict in nursing: A concept analysis. J Clinil Nurs 2023; 32: 15-6. https://doi.org/10.1111/jocn.16563 PMid:36320123 |
||||
| 25.Azoulay E, Timsit JF, Sprung CL, Soares, M, Rusinová K, Lafabrie A, et al. Prevalence and Factors of Intensive Care Unit Conflicts: the Conflicus Study. Am J Resp Crit Care Med 2009; 180: 853-60. https://doi.org/10.1164/rccm.200810-1614OC PMid:19644049 |
||||
| 26.Nayeri ND, Negarandeh R. Conflict among Iranian hospital nurses: A qualitative study. Hum Res Health 2009; 7: 25. https://doi.org/10.1186/1478-4491-7-25 PMid:19302706 PMCid:PMC2667395 |
||||
| 27.Luca CE, Sartorio A, Bonetti L, Bianchi M. Interventions for preventing and resolving bullying in nursing: A scoping review. Healthcare 2024; 12: 280. https://doi.org/10.3390/healthcare12020280 PMid:38275560 PMCid:PMC10815476 |
||||
| 28.Hirschman C. Order in the Hearing. Human Res Mag 2001; 46: .58-63. | ||||
| 29.McKenzie C. Developing a CCO (Conflict Competent Organization). Management 2002; 49: 34-6. | ||||
| 30.Zakari N, Al Khamis N, Hamadi H. Conflict and professionalism: perceptions among nurses in Saudi Arabia. Int Nurs Rev 2010; 57: 297-304. https://doi.org/10.1111/j.1466-7657.2009.00764.x PMid:20796058 |
||||
| 31.da Silva Ferreira R, Marcon GB, Rodrigues JR RA, Antunes Neto JMF, et al. Conflict management in the hospital environment and the nursing sector: A literature review. Braz J Health Rev 2024; 7: e73093. https://doi.org/10.34119/bjhrv7n5-258 |
||||
| 32.Rahim MA. A measure of styles of handling interpersonal conflict. Acad Manag J 1983; 26: 368-76. https://doi.org/10.2307/255985 |
||||
| 33.Baddari F, Salem OA, Villagracia HN. Conflict resolution strategies of nurses in a selected government tertiary hospital in the kingdom of Saudi Arabia. J Nurs Educ Pract 2016; 6: 91-9. https://doi.org/10.5430/jnep.v6n5p91 |
||||
| 34.Yılmaz F, Öztürk H. Causes of conflicts encountered by nurse managers in hospitals and their approaches in conflicts management. IUFN Hemşir Derg 2011; 19: 145-52. | ||||
| 35.Aljuaid JA, Alkarani AS. Conflict among Saudi nurses in hospitals: a qualitative study. Nurs Commun 2023; 7. https://doi.org/10.53388/IN2023015 |
||||
| 36.Alkorashy HA, Allosaimi AA, Alruwaili NF, Alshahrani SN. et al. Conflict occurrence and preferred management styles among icu nurses during the first wave of COVID‐19 pandemic: a crossover study in Saudi Arabia. Nurs Crit Care 2024; 29: 407-16. https://doi.org/10.1111/nicc.12980 PMid:37814504 |
||||
| 37.Ahmed SAEM, Gaballah S. Conflict and communication gap among the critical care nurses during care of patients with COVID-19. Int J Africa Nurs Sci 2023; 18: 100499. https://doi.org/10.1016/j.ijans.2022.100499 PMid:36313002 PMCid:PMC9597530 |
||||
| 38.Assi MD, Eshah NF. Emotional intelligence and conflict resolution styles among nurse managers: a crossover study Br J Healthcare Manag 2023; 29: 1-11. https://doi.org/10.12968/bjhc.2021.0108 |
||||
| 39. Demeubaeva DM, Kapanova GZh, Grzhibovsky AM. Strategies of nurses' behaviour in conflict situations and their influence on success in teamwork. Pharm Kazakhstan 2024; 4: 183-194. doi 10.53511/pharmkaz.2024.40.95.021 | ||||
Appendix 1.
Questionnaire
Dear colleagues!
The Kyrgyz State Medical Institute of Post-Graduate Training and Continuous Education named after S.B. Daniyarov conducts a sociological survey of medical workers of the healthcare organization on the problems of conflict, resolution of conflicts arising in labor activity and identification of the specifics of conflict management.
Instructions: Answering the questions, try to be extremely attentive and sincere. The Questionnaire is designed to be filled out easily. Please read each question of the Questionnaire in full with the answer options. Then circle those (or the one) options (option) that coincide with your opinion. If none of the proposed answer options suits you, please state your opinion on the free lines of the Questionnaire.
We will be very glad to receive your answers to the proposed questions.
THANK YOU FOR YOUR COOPERATION!
1. Your gender:
a) Male
b) Female
2. Age (y.o.):
a) 20 - 25
b) 26 - 30
c) 31 - 40
d) 41 - 59
e) 60 and older
3. Marital status:
a) Married
b) Single
4. Level of education:
a) Secondary specialized (medical school or college)
b) Tertiary (nursing)
c) Tertiary (medical) education
d) Tertiary (other)
5. Organizations you are working in:
a) Public hospital, clinic (scientific centers and institutes)
b) Private hospital/clinic
c) Family Medicine Centre
d) Other
6. Position held:
a) Deputy Nursing Director of the Healthcare Organization
b) Head Nurse
c) Senior Nurse
d) Nurse
e) Doctor
f) Head of organization, departments
7. Total length of service in the speciality (years):
a) 1 – 5 years
b) 5 – 10 years
c) 11 – 20 years
d) 20 years and over
8. Length of service in the position held (years):
a) 1 – 5 years
b) 6 – 10 years
c) 10 years and over
9. From your point of view, what is the socio-psychological climate in your organization in general?
a) Positive
b) Rather positive
c) Rather negative
d) Negative
e) It’s hard for me to say
10. How often do conflicts arise in your organization?
a) Very often
b) Occasionally
c) Sometimes
d) Almost never
e) It’s hard for me to say
11. In your opinion, conflicts between staff and patients are more common in your team?
a) Administration - staff
b) Doctor - nurse
c) Nurse - nurse
d) Senior nurse - nurse
e) Head nurse - nurse
f) Nurse - patient (sick)
g) Doctor - patient (sick)
12. What is the most common reason that pits employees against each other in your organization? (you can choose more than one reason)
a) Unfair distribution of privileges, honors, awards, bonuses and other incentives
b) Unfair labor remuneration
c) Ambitions of some employees
d) Improper organization of work
e) Peculiarities of managers’ behavior (including abuse of authority)
f) Feelings of envy among employees towards each other
g) Low level of professionalism of some employees
h) Seeking and competing for positions
i) Unclear distribution of responsibilities
j) Ineffective communication
k) Poor (lack of) working conditions
l) Non-observance of subordination and ethics of deontology
m) Human behavior (human characters)
n) Other option (please specify) ................
__________________________________________________________________________
13. Do you feel the urge to leave your organization?
a) Constantly (all the time)
b) Frequently
c) Occasionally
d) No, I don’t feel it
d) It’s hard for me to say
Please answer the questions below, assessing how typical this or that behavior is for you in a conflict situation on a five-point scale
|
No. |
Behavior |
Points |
||||
|
1 |
2 |
3 |
4 |
5 |
||
|
Never |
Rarely |
Sometimes |
Frequently |
Constantly |
||
|
1. |
I am trying to explore the problem with my colleague, and find a mutual solution acceptable to both of us |
|
|
|
|
|
|
2. |
In general, I try to meet my colleague’s needs |
|
|
|
|
|
|
3 |
I do my best not to embarrass my colleague and try to maintain confidentiality |
|
|
|
|
|
|
4. |
I try to implement my own ideas and suggestions with my colleague to make a joint decision |
|
|
|
|
|
|
5. |
I am building a relationship on the principle of “you scratch my back and I’ll scratch yours” |
|
|
|
|
|
|
6. |
I try to work with my colleague on a solution to a problem that meets our expectations. |
|
|
|
|
|
|
7. |
I usually avoid openly discussing my disagreements with my colleagues |
|
|
|
|
|
|
8. |
I usually stick to my solution to the problem encountered |
|
|
|
|
|
|
9. |
I use my influence to ensure that my ideas, suggestions and recommendations are accepted |
|
|
|
|
|
|
10. |
I will use my authority to make a decision in my favour |
|
|
|
|
|
|
11. |
I normally accept my colleague’s wishes |
|
|
|
|
|
|
12. |
I yield to my colleague’s wishes |
|
|
|
|
|
|
13. |
I have something to gain, something to lose in a conflict situation |
|
|
|
|
|
|
14. |
To solve the problem together, I share accurate information with my colleague |
|
|
|
|
|
|
15. |
Sometimes, I help my colleague make a decision in favor of his colleague. |
|
|
|
|
|
|
16. |
Normally, I yield to my colleagues |
|
|
|
|
|
|
17. |
I discuss my case with my colleague to show the merits of my position
|
|
|
|
|
|
|
Continued from page … |
||||||
|
No. |
Behavior |
Points |
||||
|
1 |
2 |
3 |
4 |
5 |
||
|
Never |
Rarely |
Sometimes |
Frequently |
Constantly |
||
|
18. |
I try to minimise our differences to reach a compromise |
|
|
|
|
|
|
19. |
I usually suggest the “golden mean” for breaking the impasse |
|
|
|
|
|
|
20. |
I am negotiating with my colleague so that a compromise can be reached |
|
|
|
|
|
|
21. |
I try to stay away from disagreements with my colleagues |
|
|
|
|
|
|
22. |
I try to avoid conflict situations with my colleague |
|
|
|
|
|
|
23. |
I use my experience to make a decision in my favour |
|
|
|
|
|
|
24. |
I often agree with my colleague’s suggestions |
|
|
|
|
|
|
25. |
I choose mutual concessions to find a compromise. |
|
|
|
|
|
|
26. |
As a rule, I hold firmly to my side of an issue |
|
|
|
|
|
|
27. |
In order to resolve the problem successfully, I try to openly express my confusion |
|
|
|
|
|
|
28. |
My colleague and I are working together to find an acceptable solution. |
|
|
|
|
|
|
29. |
I try to live up to my colleague’s expectations |
|
|
|
|
|
|
30. |
Sometimes I apply a stance, different methods to prevail in a competitive situation |
|
|
|
|
|
|
31. |
I do my best not to disclose conflict situations with my colleague so as not to hurt his/her feelings |
|
|
|
|
|
|
32. |
I try to avoid two-way unpleasant conversations with my colleagues |
|
|
|
|
|
|
33. |
I commonly avoid arguing with my colleague |
|
|
|
|
|
|
34. |
I do my best to work with my colleague on a proper understanding of the problem |
|
|
|
|
|
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
